Abstract
Sinus of valsalva aneurysm is a rare cardiac anomaly that may be congenital or acquired. We report a case of a 40-year-old male who presented with a history of acute onset exertional dyspnea. Cardiac auscultation revealed a grade IV/VI continuous murmur all over the precordium. Transthoracic echocardiography revealed sinus of valsalva arising from the right coronary sinus and alternating jet-flows into the right ventricle during different phases of the cardiac cycle suggestive of rupture of sinus of valsalva aneurysm into the right ventricle. The patient was reffered to higher centre for open-heart surgery to close the aneurysm ostium and directly suture the fistula.
Keywords: Sinus of valsalva aneurysm, sinus of valsalva aneurysm rupture, right atrium, right ventricle, continuous murmur
Sinus of valsalva aneurysm is a rare cardiac anomaly that may be congenital or acquired. It account for 1% of congenital anomalies of the heart and circulation. Especially in a newly occuring machinery murmur the existence of a sinus of valsalva aneurysm must be taken into consideration.1 It requires appropriate noninvasive examination with either echocardiography or magnetic resonance imaging to provide exact diagnosis and optimal planning of the operative procedure. A high prevalence of congenital aneurysm of sinus of valsalva is reported in Asian population. We report one such case presenting as acute heart failure and continuous murmur with diastolic accentuation, echocardiography established the diagnosis of a ruptured aneurysm of the right coronary sinus of valsalva into the right ventricle.
Case Report
A 40 year male was admitted to the emergency department of MLB Medical College Jhansi, Uttar Pradesh, India with acute onset breathlessness, palpitation and pain in upper abdomen. The patient was a laborer by occupation, chronic bidi smoker, tobacco chewer and occasional alcoholic.
Examination
Patient was of average built. His blood pressure was 110/40 mmHg in both arms in supine position. His pulse rate was 86/min, regular, bounding in character. Jugular venous pressure was markedly raised. On examination of cardiovascular system the apex beat was present in 6th intercoastal space one inch lateral to mid-clavicular line. It was hyperdynamic in character. On palpation, systolic and diastolic thrill were present over left 2nd, 3rd and 4th intercoastal space. A continuous grade IV/VI murmur with diastolic accentuation was heard all over the precordium but best heard at the base of the heart. P2 was loud and split of second heart sound was present.
The patient also had bilateral basal crepitations along with tender hepatomegaly suggestive of congestive heart failure.
Investigation
Routine lab test were within normal limits.
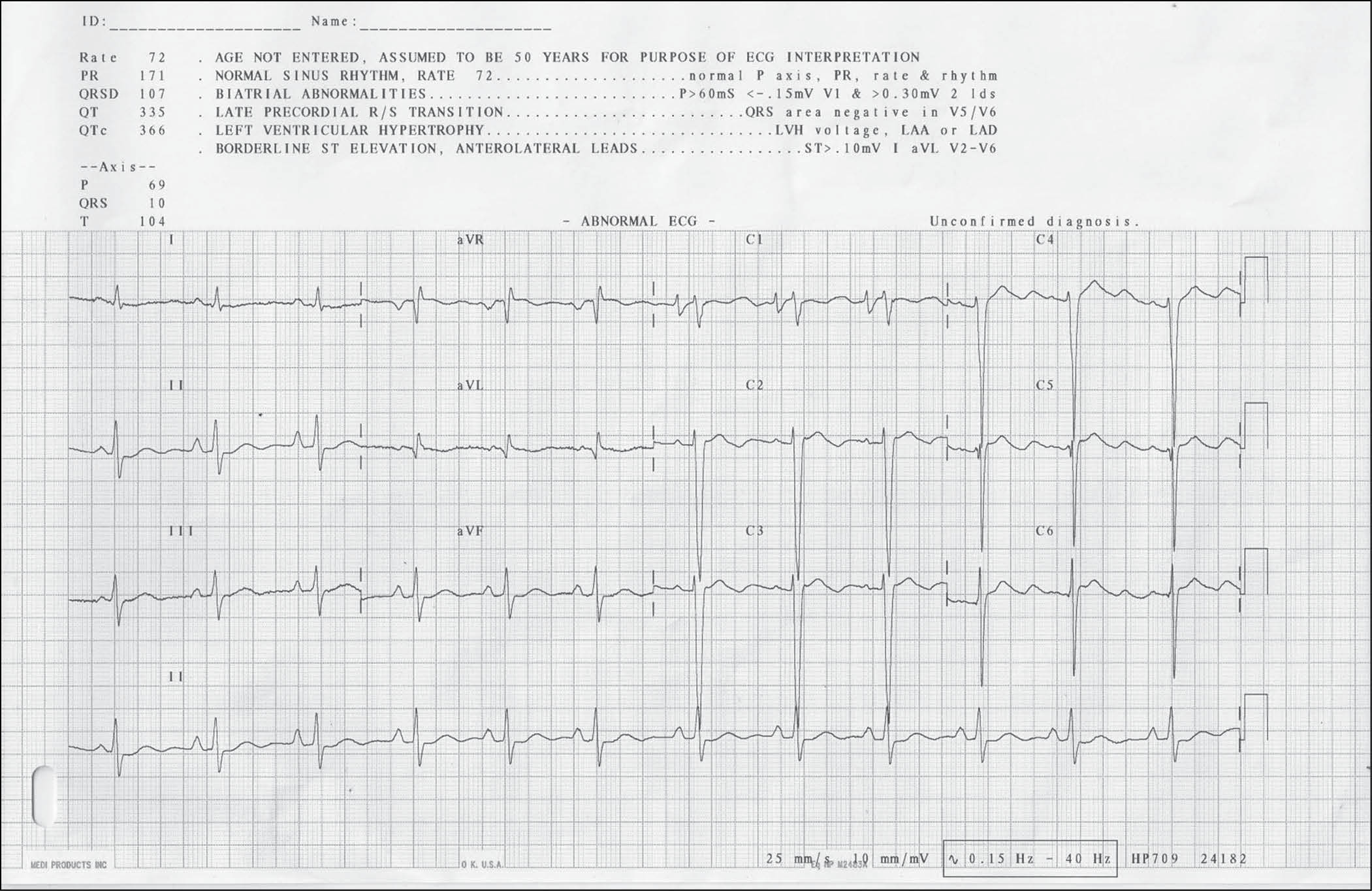
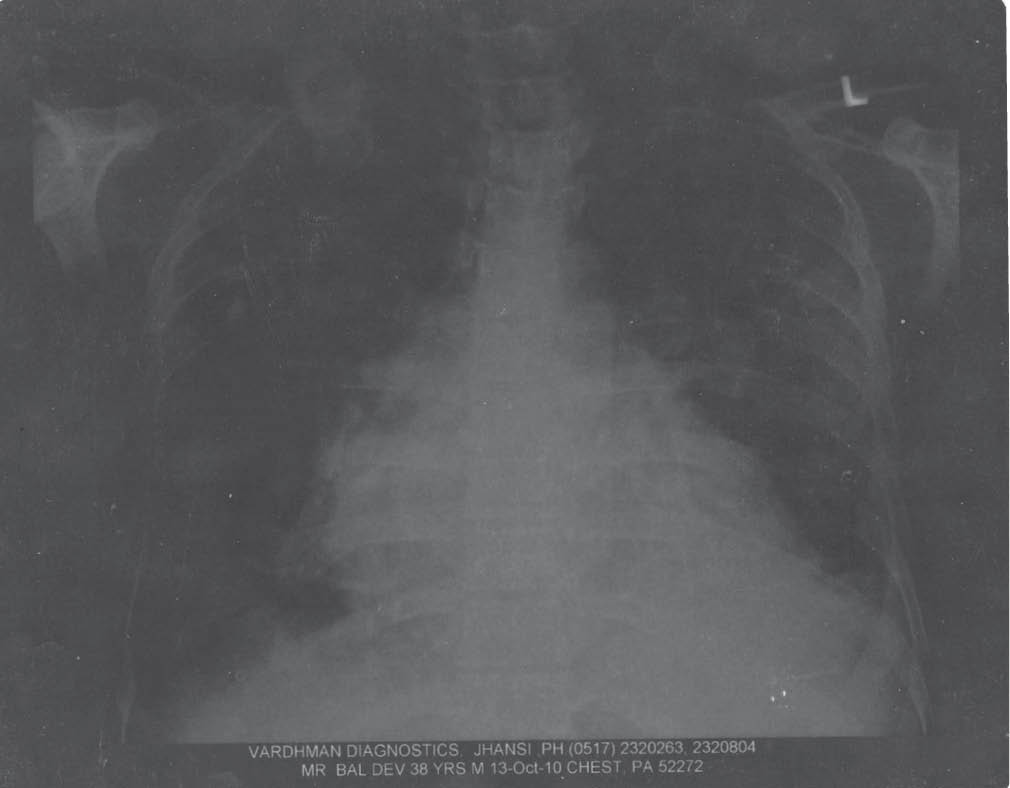
Cardiac enzymes, creatine kinase-MB (CK-MB) and troponin-I, were negative. Chest X-ray revealed cardiomegaly (Left ventricular hypertrophy, right ventricular hypertrophy, right atrial enlargement). ECG showed normal sinus rhythm with left ventricular hypertrophy with biatrial abnormality. Transthoracic echocardiography revealed sinus of valsalva arising from the right coronary sinus and alternating jet-flows into the right ventricle during different phases of the cardiac cycle suggestive of rupture of aneurysm into the right ventricle.
The patient was managed medically with full treatment for acute heart failure but without much relief. The patient was subsequently referred to higher centre for operative procedure where he still awaits treatment.
Discussion
The sinus of valsalva are 3 small out pouchings in the wall of aorta immediately above the attachment of each aortic cusp. They are named as either the right coronary sinus, the left coronary sinus and the noncoronary sinus depending on their relationship to the coronary arteries. Congenital sinus of valsalva aneurysm is caused by a dilatation, usually of a single sinus of valsalva from a separation between the aortic media and the annulus fibrosis. 90-95% originate in the right or noncoronary sinus and project into the right ventricle or right atrium, leaving less than 5% that originate in the left coronary sinus. Those arising in the right coronary sinus rupture into the right ventricle or occasionally into right atrium. Those arising in the noncoronary sinus almost all rupture in right atrium. As discussed these rare aneurysms are eventually diagnosed once they rupture, typically fistulazing into another cavity (pericardium, atrium, right ventricle, or right outflow tract) and manifesting symptoms and signs.2 In our patient too, sinus of valsalva was arising from right coronary sinus and get rupture into right ventricle leading to symptoms of heart failure, which is the most common site of origin and rupture as described in literature. Associated anomalies are common and include ventricular septal defect (VSD) (50%), aortic regurgitation (20%) and coarctation of aorta.3 In our patient no associated anomalies were seen. Rupture of aneurysm sac may occur spontaneously or may be precipitated by exertion, trauma or cardiac catheterization. In our case it occured spontaneously. Ruptured congenital sinus of valsalva aneurysm occur chiefly in males, with a sex ratio as high as 4:1. Rupture usually occurs in young men before 30 years of age leading to sudden congestive heart failure because the heart cannot rapidly adapt to hemodynamic burden. Our case was too male but presentation occur slightly later age at 40 years. Death usually follows within a year after rupture.4 Unruptured aneurysm may come to notice by:
- To-and-fro murmur due to flow in and out of the intact aneurysmal pouch.
- Midsystolic murmur caused by obstruction to right ventricular outflow tract.
- Myocardial ischemia due to coronary artery compression.
- Aortic regurgitation caused by malposition of aortic cusps.
- Superior vena cava obstruction.
- Paracardiac mass in chest X-ray.
- Systemic emboli.
- Complete heart block.
- Sudden death.
As stated by Ming-Shyan Lin, et al (2009)5 in a interesting case report, in rupture of sinus of valsalva the murmurs are loud, and continuous; they vary in intensity during systole and diastole, and are best heard at the base of the heart. The murmurs start in the systole and continue to be in diastole, peaking near S2. The intensity of the murmurs may be diminished at around the second heart sound, only to increase again during diastole, creating a ‘to-and-fro’ cadence. In our patient too murmur was continuous with a diastolic accentuation best heard at the base of the heart. Possible differential diagnoses in these cases include patent ductus arteriosus, cervical venous hum, mammary soufflé of pregnancy, anomalous origin of coronary arteries from great vessel, or hemodialysis arteriovenous fistulas.
In the present case patient is young male presenting with acute onset of heart failure with continuous murmur without any history of rheumatic and ischemic heart disease, compelled us to think in the direction of rupture of sinus of valsalva. In a case study by Sakakibara, et al (1962)6 rupture of sinus of valsalva into the right atrium or right ventricle results in volume overload of both ventricles, but the electrocardiogram usually shows left ventricular hypertrophy by voltage criteria and ST segment and T wave abnormalities. In our case too patients ECG showed normal sinus rhythm with left ventricular hypertrophy with biatrial abnormality consistent with above findings.
Conclusion
The main aim of our case report is that due to high prevalence of congenital aneurysm of sinus of valsalva in Asian population in comparision to western counterpart, inspite of rare presentation, we must rule out rupture of sinus of valsalva in a previously healthy, young adult, usually male, presenting with a loud continuous murmur and acute cardiac failure. Surgery is the definitive therapy for sinus of valsalva aneurysm. Depending on the clinical presentation, perioperative medical management consists of (1) relieving heart failure symptoms, (2) treating arrhythmia (if present), and (3) treating endocarditis (if present).
References
- Wells T, Byrd B, Neirste D, Fleurelus C. Sinus of valsalva aneurysm with rupture into the interventricular septum and left ventricular cavity. Circulation. 1999;100 (17):1843-4.
- Feldman DN, Roman MJ. Aneurysms of the sinuses of valsalva. Cardiology. 2006;106(2):73-81.
- Wang ZJ, Fan QX, Zou CW, Li DC, Li HX, Wang AB, et al. Clinical analysis for 70 sinus of valsalva aneurysm. Zhonghua Wai Ke Za Zhi. 2004;42(13):808-11.
- Moustafa S, Mookadam F, Cooper L, Adam G, Zehr K, Stulak J, et al. Sinus of valsalva aneurysms-47 years of a single center experience and systematic overview of published reports. Am J Cardiol. 2007;99(8):1159-64.
- Ming-Shyan Lin, Chia-Pin Lin, Jaw-Ji Chu, Yuan-Chang Liu, Pao-Hsien Chu. Rupture of right sinus of valsalva aneurysm with alternating shunting into right atrium and right ventricle. Acta Cardiol Sin. 2009;25:52-5.
- Sakakibara S, Konno S. Congenital aneurysms of sinus of valsalva. A clinical study. Am Heart J. 1962;63:708-19.